矯正用アンカースクリューで治療期間は本当に短くなるの?を解説しよう
なりません(解散)。
矯正治療を検討中の方から、「できるだけ早く治療を終わらせたいのですが、良い方法はありませんか?」というご相談をよくいただきます。その中で、「アンカースクリュー(ミニスクリュー/TAD)を使えば、治療期間が劇的に短くなるとネットで見たのですが……」と質問されることがたまにあります。
「アンカースクリューを使いたい。アンカースクリューが使える医院で矯正したい」と一昨年はよく聞かれた記憶が有りますが。その度に「アンカースクリューを使ってたからといって治療期間が短くなることはない」と否定していました。と思ったら自院のブログにもそう書いてあったりして書いたの誰だよって思いましたが…
確かに、アンカースクリューは現代の矯正歯科において画期的な装置です。しかし、「誰でも全体の治療期間が魔法のように半分になる」といった認識は、実は誤解を含んでいます。
今回は、論文データに基づき、アンカースクリューの「本当の目的」と「治療期間に与える影響」について検討してみましょう。
1. 結論:「全体の治療期間」が劇的に短縮されるわけではない
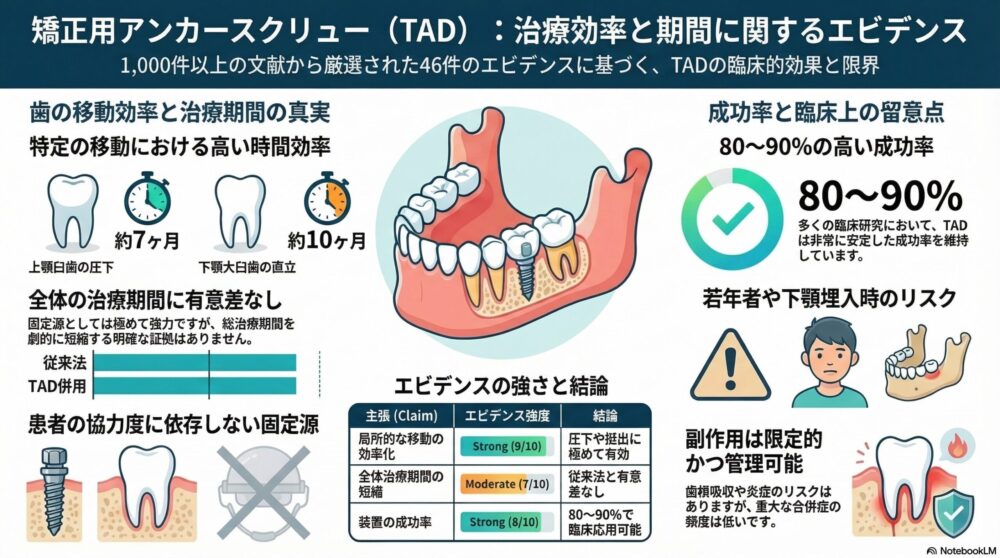
まず結論から。アンカースクリューを使用したからといって、矯正治療の全体の期間が大幅に短縮されるという明確な医学的根拠(エビデンス)は、現在のところ限定的です 。
実際に複数の臨床研究をまとめたデータでも、アンカースクリューなどの外科的な固定源は、従来の方法と比べて全体の治療期間に有意な差をもたらさないと報告されています 。一部の研究では、最も強力な固定源であるにもかかわらず、従来の装置(Nanceのホールディングアーチなど)よりも総治療期間が長くなる傾向があったとする報告すらあります 。
歯を動かすスピードには、骨の代謝という「生物学的な限界」があります。強い力をかければ早く動くわけではなく、無理な力をかけると歯根吸収などのトラブルにつながります。そのため、安全に歯を動かせるペースは、どのような装置を使っても劇的には変わらないのです。
2. アンカースクリューの本当の役割は「絶対的な固定源」
では、なぜ私たちがアンカースクリューを推奨するケースがあるのでしょうか? その最大の理由は、「患者さんの協力に依存しない、絶対に動かない固定源(足場)を作れること」にあります 。
歯を動かすメカニズムは「綱引き」に似ています。前歯を後ろに下げたい時、奥歯を支えにして引っ張りますが、その反作用で奥歯も前へ引っ張られてしまいます。アンカースクリューを用いたとしても歯の移動は作用-反作用の原則から逃れられるわけではありません。
従来は、奥歯が前に来ないようにヘッドギアなどの学外固定装置を患者さんご自身で毎日装着していただく必要がありました。しかし、これでは「装着時間(協力度)」によって治療の進行が大きく左右されてしまいます 。 アンカースクリューを顎の骨に小さなネジとして埋め込むことで、これが「絶対に動かない杭」となり、奥歯に負担をかけず、協力度に依存せず理想的な方向へ歯を引っ張ることが可能になるのです 。
3. 「部分的な歯の移動」には圧倒的なスピードと効率を発揮する
全体の期間は変わらなくても、「局所的な歯の移動(特定の歯だけを大きく動かすこと)」においては、アンカースクリューは圧倒的な効率化をもたらします 。
従来の方法では難易度が高く、外科手術が必要だったような歯の動きも、以下のようにスムーズに行えるようになりました。
- 奥歯を顎の骨に押し込む動き(圧下): 開咬(前歯が噛み合わない状態)やガミースマイルの改善に有効です。最新のデータでは、アンカースクリューを用いることで平均約6.9〜7.1ヶ月で効率的に奥歯を押し込めることが分かっています 。
- 倒れてしまった奥歯を起こす動き: 手前に大きく倒れ込んだ下顎の第二大臼歯(一番奥の歯)を正しい位置に直立させる(アップライト)治療も、約10ヶ月程度で効果を発揮するという報告があります 。
このように、「特定の難しい動き」をスムーズにクリアできるという点において、アンカースクリューは非常に大きなメリットがあります。
4. 治療を受ける前に知っておきたい成功率とリスク
医療である以上、メリットだけでなくリスクも正しくお伝えすることが私たちの責任です。
アンカースクリューの成功率は80〜90%前後と高く、臨床において十分に信頼できる治療法です 。 しかし、100%ではありません。例えば、骨がまだ柔らかい若年者の患者様や、下顎に埋め込む場合などは、ネジが抜けやすくなる(失敗リスクが上がる)傾向があります 。また、大きな合併症の頻度は低いものの、一時的な歯茎の炎症などが起こる可能性はゼロではありません 。
どうしても全体の治療期間自体を短縮したいという方には、歯の周りの骨に外科的なアプローチを行う治療法(コルチコトミー)もありますが、コルチコトミー併用矯正が出来る医院は極々少数です。
5. まとめ:患者さんも勉強する時代
アンカースクリューは、「誰でも早く治療が終わる魔法のネジ」ではありません。しかし、患者さんの負担を減らし、従来は難しかった精密な歯のコントロールを可能にする強力なサポーターです。
大体、広告に力を入れている医院は「耳障りの良い言葉」を並べて自分がやりたい治療に誘導するものです。ネット上の噂や流行りに流されることなく、正しい情報を得るために患者さんも勉強する時代です。
Deguchi, T., Takano-Yamamoto, T., Kanomi, R., Hartsfield, J., We, R., & Garetto, L. (2003). The Use of Small Titanium Screws for Orthodontic Anchorage. Journal of Dental Research, 82, 377 – 381. https://doi.org/10.1177/154405910308200510
Yin, Y., Wang, Z., Huang, L., Zhao, Y., Guan, Q., Xu, H., & Han, X. (2021). Orthodontic maximum anchorages in malocclusion treatment: A systematic review and network meta‐analysis. Journal of Evidence‐Based Medicine, 14, 295 – 302. https://doi.org/10.1111/jebm.12453
Manea, A., Dinu, C., Băciuț, M., Buduru, S., & Almășan, O. (2022). Intrusion of Maxillary Posterior Teeth by Skeletal Anchorage: A Systematic Review and Case Report with Thin Alveolar Biotype. Journal of Clinical Medicine, 11. https://doi.org/10.3390/jcm11133787
Sbricoli, L., Ricci, S., Cattozzo, A., Favero, R., Bressan, E., & Sivolella, S. (2022). Mandibular Molar Uprighting Using Skeletal Anchorage: A Novel Approach. Journal of Clinical Medicine, 11. https://doi.org/10.3390/jcm11133565
Mezio, M., Altieri, F., & Cassetta, M. (2024). Skeletal Anchorage as a Therapeutic Alternative for Mandibular Second Molar Impaction: A Prospective Case–Control Study. Dentistry Journal, 12. https://doi.org/10.3390/dj12110359
Reynders, R., & Isaia, L. (2019). Failure rates of palatal implants or mini-screws for orthodontic anchorage. Evidence-Based Dentistry, 20, 9-11. https://doi.org/10.1038/s41432-019-0010-0
Jang, W., Byun, S., Cho, S., Park, I., Yi, S., Kim, J., & Yang, B. (2021). Correction of Condylar Displacement of the Mandible Using Early Screw Removal following Patient-Customized Orthognathic Surgery. Journal of Clinical Medicine, 10. https://doi.org/10.3390/jcm10081597
Uribe, F., Padala, S., Allareddy, V., & Nanda, R. (2014). Patients’, parents’, and orthodontists’ perceptions of the need for and costs of additional procedures to reduce treatment time.. American journal of orthodontics and dentofacial orthopedics : official publication of the American Association of Orthodontists, its constituent societies, and the American Board of Orthodontics, 145 4 Suppl, S65-73. https://doi.org/10.1016/j.ajodo.2013.12.015
Michelogiannakis, D., Jabr, L., Barmak, A., Rossouw, P., Kotsailidi, E., & Javed, F. (2021). Influence of low-level-laser therapy on the stability of orthodontic mini-screw implants. A systematic review and meta-analysis.. European journal of orthodontics. https://doi.org/10.1093/ejo/cjab016
Lee, H., Lee, S., Park, J., Lee, J., Chung, C., Lee, K., Yu, H., & Kim, K. (2025). Periodontal changes in supraerupted maxillary molars after orthodontic intrusion using miniscrews: A retrospective study.. American journal of orthodontics and dentofacial orthopedics : official publication of the American Association of Orthodontists, its constituent societies, and the American Board of Orthodontics. https://doi.org/10.1016/j.ajodo.2025.05.005
Kazimierczak, N., Kazimierczak, W., Serafin, Z., Nowicki, P., Nożewski, J., & Janiszewska-Olszowska, J. (2024). AI in Orthodontics: Revolutionizing Diagnostics and Treatment Planning—A Comprehensive Review. Journal of Clinical Medicine, 13. https://doi.org/10.3390/jcm13020344
Chen, Y., Chang, H., Huang, C., Hung, H., Lai, E., & Yao, C. (2007). A retrospective analysis of the failure rate of three different orthodontic skeletal anchorage systems.. Clinical oral implants research, 18 6, 768-75. https://doi.org/10.1111/j.1600-0501.2007.01405.x
Reynders, R., & Lange, J. (2014). Moderate quality evidence that surgical anchorage more effective than conventional anchorage during orthodontic treatment. Evidence-Based Dentistry, 15, 108-109. https://doi.org/10.1038/sj.ebd.6401060
Stanford, N. (2011). Mini-screws success rates sufficient for orthodontic treatment. Evidence-Based Dentistry, 12, 19-19. https://doi.org/10.1038/sj.ebd.6400777
Fanouriakis, A., Kostopoulou, M., Andersen, J., Aringer, M., Arnaud, L., Bae, S., Boletis, J., Bruce, I., Cervera, R., Doria, A., Dörner, T., Furie, R., Gladman, D., Houssiau, F., Inês, L., Jayne, D., Kouloumas, M., Kovács, L., Mok, C., Morand, E., Moroni, G., Mosca, M., Mucke, J., Mukhtyar, C., Nagy, G., Navarra, S., Parodis, I., Pego-Reigosa, J., Petri, M., Pons-Estel, B., Schneider, M., Smolen, J., Svenungsson, E., Tanaka, Y., Tektonidou, M., Teng, Y., Tincani, A., Vital, E., Van Vollenhoven, R., Wincup, C., Bertsias, G., & Boumpas, D. (2023). EULAR recommendations for the management of systemic lupus erythematosus: 2023 update. Annals of the Rheumatic Diseases, 83, 15 – 29. https://doi.org/10.1136/ard-2023-224762
Qiu, L., Xu, H., Feng, P., Sha, X., & Zhang, H. (2021). Clinical effectiveness of orthodontic miniscrew implantation guided by a novel cone beam CT image-based computer aided design and computer aided manufacturing (CAD-CAM) template. Annals of Translational Medicine, 9. https://doi.org/10.21037/atm-21-2575
Kuroda, S., & Tanaka, E. (2014). Risks and complications of miniscrew anchorage in clinical orthodontics. Japanese Dental Science Review, 50, 79-85. https://doi.org/10.1016/j.jdsr.2014.05.001
Alhamwi, A., Burhan, A., Idris, M., & Nawaya, F. (2024). Duration of orthodontic treatment with clear aligners versus fixed appliances in crowding cases: a systematic review. Clinical Oral Investigations, 28. https://doi.org/10.1007/s00784-024-05629-y
Seiryu, M., Ida, H., Mayama, A., Sasaki, S., Sasaki, S., Deguchi, T., & Takano-Yamamoto, T. (2019). A comparative assessment of orthodontic treatment outcomes of mild skeletal Class III malocclusion between facemask and facemask in combination with a miniscrew for anchorage in growing patients: A single-center, prospective randomized controlled trial.. The Angle orthodontist. https://doi.org/10.2319/101718-750.1
Topouzelis, N., & Tsaousoglou, P. (2012). Clinical factors correlated with the success rate of miniscrews in orthodontic treatment. International Journal of Oral Science, 4, 38 – 44. https://doi.org/10.1038/ijos.2012.1
Lai, E., Yao, C., Chang, J., Chen, I., & Chen, Y. (2008). Three-dimensional dental model analysis of treatment outcomes for protrusive maxillary dentition: comparison of headgear, miniscrew, and miniplate skeletal anchorage.. American journal of orthodontics and dentofacial orthopedics : official publication of the American Association of Orthodontists, its constituent societies, and the American Board of Orthodontics, 134 5, 636-45. https://doi.org/10.1016/j.ajodo.2007.05.017
Nakawah, S., Youssef, M., Rossi, O., Perrotti, G., & Testori, T. (2025). The Effect of the I-Arch on the Buccal Alveolar Crest in Comparison with the Traditional Archwire Sequence: A Randomized Controlled Clinical Trial. Journal of Clinical Medicine, 14. https://doi.org/10.3390/jcm14031026
Luzzi, V., Fioravanti, M., Mitrano, L., Marasca, B., Saccucci, M., Celli, M., Celli, L., Vozza, I., & Ierardo, G. (2024). Orthodontic Management in Pediatric Patients with Rare Diseases: Case Reports. Journal of Clinical Medicine, 14. https://doi.org/10.3390/jcm14010055
Zhou, H., Zhang, Y., Qi, Y., Zhang, Q., Liu, N., & Chen, Y. (2024). The efficacy and safety of corticotomy and periodontally accelerated osteogenic orthodontic interventions in tooth movement: an updated meta-analysis. Head & Face Medicine, 20. https://doi.org/10.1186/s13005-024-00409-1
監修者

中嶋 亮 | Ryo Nakajima
日本大学松戸歯学部卒業後、同大学大学院にて歯科矯正学を専攻し修了。大学病院での研鑽を経て、2012年より「銀座矯正歯科」に勤務し、数多くの裏側矯正や複雑な症例に携わる。2021年に院長、現在は理事長として診療にあたる。見た目の美しさと咬合機能の両立を重視し、特に舌側矯正やデジタル技術を活用した精密治療に注力。患者一人ひとりの生活背景に寄り添い、長期的な健康と自然な笑顔を引き出すことを理念としている。
【略歴】
- 1998年 富山県立富山中部高等学校卒業
- 1998〜2004年 日本大学松戸歯学部
- 2004〜2008年 日本大学大学院(歯科矯正学専攻)
- 2008〜2012年 日本大学松戸歯学部 歯科矯正学講座 助手(専任扱)
- 2012〜2020年 医療社団法人真美会 銀座矯正歯科 アシスタントドクター
- 2013〜2014年 ニューヨーク大学CDEP 矯正学修了
- 2014〜2018年 日本大学松戸歯学部 顎顔面外科学講座 兼任講師
- 2014〜2015年 カリフォルニア州立大学LA校CDEP 矯正学修了
- 2019〜2023年 日本大学松戸歯学部 歯科矯正学講座 兼任講師
- 2021年〜 医療社団法人真美会 銀座矯正歯科 院長
- 2022年〜 日本デジタル矯正歯科学会 理事・学術担当
- 2023年〜 日本大学松戸歯学部 歯科矯正学講座 クリニカルアドバイザー
- 2023年〜 Digital Dentistry Society Ambassador (Japan)
- 2023年〜 日本大学松戸歯学部 歯科矯正学講座 同門会副会長
- 2023年〜 RayFace (RayDent, Korea) Key Opinion Leader
- 2024年〜 医療法人社団真美会 理事長
【主な所属学会】
- ・日本矯正歯科学会(認定医)
- ・International Congres of Oral Implantrogists (ICOI) インプラント矯正認定医
- ・Digital Dentistry Society 日本アンバサダー
- ・先進歯科画像研究会(ADI) 歯科用CT認定医
- ・厚生労働省認定 歯科臨床研修指導医
- ・日本美容外科学会(JSAPS) 関連会員
- ・Orthopaedia and Solutions マネージャー
- ・(株)YDM 矯正器材アドバイザー
- ・ABO Journal Club 主宰
- ・Cutting Edge of Digital Orthodontics 主宰
- ・BiTechOrtho代表
- ・Orthodontics Institute Japan代表
【論文・学会発表】
- ・加速矯正とアライナー治療による治療期間のコントロール ザ・クインテッセンス2022年11月号
- ・進化するデジタル歯科技術Extra モディファイドコルチコトミー法とSureSmileによる矯正治療 日本歯科評論 81(8)=946:2021.8
- ・進化するデジタル歯科技術 : 3Dプリンターは臨床をどう変革するか(4)矯正治療における3Dプリンターの臨床応用 日本歯科評論 81(4)=942:2021.4
- ・矯正用光重合型レジン系接着システムの接着性能 接着歯学2013年31巻4号P159-166
- ・歯科矯正学における3D診断および治療計画(翻訳) クインテッセンス出版
- ・基礎から学ぶデジタル時代の矯正入門(翻訳統括) クインテッセンス出版
- ・矯正歯科治療のためのコルチコトミー(翻訳)
- ・Effects of… cells in vitro. J Periodontal Res. 2008 Apr;43(2):168-73.
- ・Evaluation…lary tuberosity. J World Fed Orthod. 2022 Jun;11(3):69-74.
- ・T-helper 1…essive orthodontic forces. Oral Dis. 2012 May;18(4):375-88
- ・IL-8 and M…s in periodontal tissues. Oral Dis. 2011 Jul;17(5):489-98.
- ・Effects of…dontal ligament cells. Inflamm Res. 2011 Feb;60(2):187-94.
- ・Effects of…igament cells. Orthod Craniofac Res. 2009 Nov;12(4):282-8.
- ・Levels of …cells in vitro. Orthod Craniofac Res. 2006 May;9(2):63-70.
- ・日本デジタル歯科学会招待講演(2024年)
- ・東北矯正歯科学会招待講演(2025年)
- ・加速矯正による治療期間短縮のコンセプト クインテッセンス出版
- ・Levels of …cells in vitro. Orthod Craniofac Res. 2006 May;9(2):63-70.